
History and Physical
Chief Complaint: “The right side of my stomach has been hurting for an hour”
History of Present Illness:
D.A. is a 65 y/o F w/ a PMHx HTN, T2DM, Sjogren’s syndrome, arthritis, osteoporosis, cataracts, and malignant neoplasm of upper outer quadrant of LT breast. She presents to the ED in the evening hours of 01/02 for sudden, severe 10/10 RLQ pain radiating to the lower back x1 hour. She reports that the pain began shortly after she had dinner which consisted of boiled green plantains with fried eggs, fried salami, and avocado. The pain is described as sharp, cramping, and steady since onset. Patient states that pain is aggravated by inhaling too deeply, denies any alleviating factors, and did not take any medication for the pain. Last bowel movement and flatus was in the early morning hours on 01/02. Last endoscopy was performed June 30, 2023, results unremarkable. Patient denies fever, chills, shortness of breath, recent travel, chest pain, changes in appetite, history of similar symptoms, trauma, dysuria, urinary urgency, urinary frequency, dysuria, hematuria, vaginal bleeding/discharge, hematochezia, and melena.
Past Medical History:
HTN diagnosed x12 years ago, managed by primary care provider at Woodhull
T2DM diagnosed x4 years ago, managed by endocrinologist at Woodhull
GERD diagnosed x5 years ago, managed by gastroenterologist at NYU Langone
Scleroderma diagnosed x4 years ago, managed by rheumatologist at Woodhull
Arthritis diagnosed x8 years ago, managed by rheumatologist at Woodhull
Osteoporosis diagnosed x5 years ago, managed by endocrinologist at Woodhull
Bilateral cataracts 2 years ago, managed by ophthalmologist at private clinic
Malignant neoplasm of upper outer quadrant of LT breast (LT papillary carcinoma/DCIS) x7 years ago, managed by oncologist at Woodhull, currently in remission and not taking any medication for condition
Immunization History:
All immunizations are up to date including COVID-19 (2022), influenza (2023), and pneumococcal (2024); patient vaccinated against TB with BCG in the Dominican Republic during adolescence
Preventative Medicine Screening:
Mammography – November 01, 2023; no significant masses, calcifications, or other findings seen in either breast. Scar marker overlies the LT breast
Pap Smear – August 28, 2023; normal
Bone Density/DEXA Scan – December 06, 2023; scores fell within one SD
Endoscopy – grade A esophagitis with non-obstructive Schatzi ring
Colonoscopy – June 2023; normal
Dental – February 2024; patient’s dentures assessed, dentures are properly fitting
Ophthalmologic – March 2024; b/l cataracts not impairing activities or lifestyle
Past Surgical History:
Lumpectomy of the LT breast performed at Woodhull in 2018
Open caesarian section in El Hospital Regional De San Vicente Paul en San Francisco de Macoris, 1990, uncomplicated
Medications:
Home Medications:
- Nifedipine ER 24 hr tablet 60 mg PO daily for HTN
- Pantoprazole 40 mg BID PO daily for GERD
- Alendronate one 70mg tablet PO every 7days for osteoporosis
- Metformin 1,000 mg PO BID for T2DM
- Zolpidem 10 mg PO nightly PRN for sleep
Hospital Medications:
- Cefoxitin 2,000 mg in dextrose 5% water 100 mL IVPB every 8 hours @ 200 mL/hr over 30 minutes for cholecystitis
- Enoxaparin subcutaneous injection 40 mg for DVT prevention
- Insulin Aspart Injection 0-8 Units TID PRN 5-15 minutes before meals for T2DM if blood sugar is:
- Between 181-220; administer 2 units
- Between 221-260; administer 3 units
- Between 261-300; administer 4 units
- Between 201-350; administer 5 units
- > 350; administer 6 units and notify provider
- Nifedipine ER 24 hr tablet 60 mg PO daily for HTN
- Famotidine injection 20 mg IV push once daily for GERD
- Pantoprazole injection 40 mg IV push once daily for stress ulcer prophylaxis
- Ketorolac 15 mg injection every 6 hours as needed for pain; do not exceed 120 mg in 24 hours
- 1 mg & dextrose (D50W) 50% water injection 25 mg IV push for blood glucose < 70 mg/dL
- Glucagon injection for blood glucose < 70 mg/dL
- Ondansetron injection 4 mg every 6 hours PRN for nausea and vomiting
Allergies:
NKDA
No known food allergies
No known environmental allergies
Family History:
Mother is deceased, age 93, PMHx breast cancer (type unknown), HTN, and T2DM
Father is deceased, age 87, PMHx HTN and hypercholesterolemia
Older sister is deceased, age 57 PMHx colorectal CA
Daughter who is alive and well, age 34, PMHx HTN and hypercholesterolemia, resides in Connecticut and is patient’s main support system
Son, who is alive and well, age 37, no PMHx, resides in the Dominican Republic; visits twice a year
Social History:
D.A. is a 65 y/o Hispanic female domiciled in Brooklyn, New York. Lives alone and does not have pets. She performs her ADLs and IADLs without assistance. She will be returning to her apartment which is located on the first floor.
Habits – denies any EtOH consumption or illicit drug use; was a former smoker with 20 pack years, quit in 2017
Travel – no recent travel
Diet – for breakfast patient has black coffee, no sugar or milk. For lunch she has chicken, turkey or tuna with rice. For dinner she has green plantains or bananas with fried egg, fried salami, and avocado. Will snack on fruit such as apples, blueberries, and strawberries throughout the day
Exercise – patient performs weight bearing exercises at home; she also walks about 1-2 miles a day.
Sleep – sleeps 7-8 hours a night, uninterrupted
Safety measures – practices seatbelt safety measures
Sexual Hx – not sexually active
Occupation – used to work a front desk job in the Dominican Republic
PCP – Shah Sapana, MD
Pharmacy – Avon Pharmacy on 82 Graham Avenue
Proxy – patient’s daughter
Review of Systems:
General: Denies fever, chills, night sweats, fatigue, weakness, loss of appetite, recent weight gain or loss
Skin, hair, nails: Denies changes in texture, excessive dryness or sweating, discolorations, pigmentations, moles/rashes, pruritus, changes in hair distribution
HEENT: Denies headache, vertigo, head trauma, unconsciousness, coma, use of contacts, glasses, visual disturbances, fatigue, lacrimation, photophobia, deafness, pain, discharge, tinnitus, use of hearing aids, nasal discharge, epistaxis, bleeding gums, sore tongue, sore throat, mouth ulcers, voice changes, dentures
Neck: Denies localized swelling/lumps, stiffness/decreased range of motion
Breast: Denies lumps, nipple discharge, pain
Pulmonary system: Denies dyspnea, SOB, cough, wheezing, hemoptysis, cyanosis, orthopnea, PND
Cardiovascular system: Reports hx HTN. Denies chest pain, palpitations, irregular heartbeat, edema/swelling of ankles or feet, syncope, known heart murmur
Gastrointestinal system: as per HPI
GU/GYN: Frequency: 4-5 times a day. color of urine: clear/yellow. Denies urinary incontinence, dysuria, nocturia, urgency, oliguria, polyuria. Date of last normal period: two years ago, March. Age of menarche: 12 y/o; G:2 T:2 P:0 A:0 L:2
Sexual history: Sexually active? No. Tested positive for chlamydia in her 30’s.
Musculoskeletal System: Denies muscle/joint pain, deformity or swelling, redness, arthritis
Peripheral Vascular System: Denies intermittent claudication, coldness of trophic changes, varicose veins, or peripheral edema
Hematologic System: Denies easy bruising or bleeding, lymph node enlargement, hx of clot
Endocrine System: Denies polyuria, polydipsia, polyphagia, heat or cold intolerance, goiter, hirsutism
Nervous System: Denies seizures, loss consciousness, ataxia, loss of strength, change in cognition/mental status/memory, weakness (asymmetric)
Psychiatric: Reports hx of depression and anxiety in 2017, obsessive/compulsive disorder, have you ever seen a mental health professional? Yes. Medications: buspirone and citalopram; both d/c in 2021. Denies hx OCD
Vital Signs:
Temperature: 98.1
O2 Sat: 95
Height: 63 inches
Weight: 61.2 kg
BMI: 23.9 kg/m2
Respiratory Rate: 17
Heart Rate: 60
Blood Pressure: 123/74
Physical:
General: Patient appears clean & well groomed, alert & oriented to time, place, and person. Is lying in bed reading a book. Appears stated age and is not in acute distress.
Hair, Head, and Face:
Hair is of average quantity and distribution. Brown/gray in color with curly texture.
Head is normocephalic, and atraumatic. Face is symmetrical with no signs of drooping, swelling, or trauma.
Skin, and Nails:
The skin is warm and moist with good turgor. Non-icteric with no swelling or signs of ecchymosis. Patient has a 2cm x 3cm pink heart tattoo on RT wrist.
Eye:
The eyes are symmetrical OU. Conjunctiva is pink, sclera is white. The pupils and iris are round. There is no exophthalmos OU. PERRLA, EOMs intact.
Ear:
Symmetrical and appropriate in size. No lesions, masses, or trauma on external ears.
Nose and Sinus:
The nose is symmetrical without masses, deformities, trauma, or discharge.
Mouth and Pharynx:
The lips are pink with no signs of blisters, fissuring, or cyanosis.
The buccal mucosa is pink and well hydrated.
The tongue is pink and covered in papillae with no signs or leukoplakia.
The gingiva is pink. No hyperplasia, erythema, masses, lesions, or bleeding.
There is no tonsillar adenopathy, the uvula is pink, moist, and midline.
Patient is wearing properly fitting dentures.
Neck, Thyroid, and Lymph Nodes:
The trachea is midline without masses or scars.
Cardiac:
Regular rate and rhythm. Normal S1 and S2, no murmurs, S3, S4, friction rubs, or gallops noted.
Thorax and Lung:
Chest is symmetrical with no signs of deformity, or trauma. Respirations are unlabored without use of any accessory muscles. Patient has good airflow. No wheezing, rhonchi, or rales noted.
Abdomen:
Abdomen is flat, soft, non-distended. There is abdominal tenderness in the RUQ on light and deep palpation. Positive signs include McBurney’s sign. Pfannenstiel incision scar well-approximated and well-healed without any evidence of appreciable masses around or underneath it.
Neurologic Exam:
Alert & oriented to person, place, and time. Intact attention, cooperative, coherent thought, & speech.
Peripheral Vascular Exam:
The extremities are normal in color, size and temperature. Pulses are 2+ bilaterally in upper and lower extremities. No bruits noted. No clubbing, cyanosis or edema noted bilaterally. No stasis changes or ulcerations noted. No calf tenderness bilaterally. No palpable cords or varicose veins bilaterally.
MSK Upper/Lower Extremity:
No soft tissue swelling / erythema / ecchymosis / atrophy / or deformities in bilateral upper and lower extremities. Non-tender to palpation / no crepitus noted throughout. FROM of all upper and lower extremities bilaterally.
DDx:
- Cholecystitis
- Acute Appendicitis
- Renal Colic s/t nephrolithiasis
Laboratory Findings 06/04-06/05
CMP w/ Magnesium & Phosphate CBC w/ Differential
| Anion Gap | 16 | WBC | 7.44 | Basophil % | 0.5 | ||
| Sodium | 136 | RBC | 4.98 | Basophil Abs | 0.04 | ||
| Potassium | 4.1 | HGB | 12.7 | Imm Gran Abs | 0.02 | ||
| Chloride | 98 | HCT | 39.8 | Imm Gran % | 0.3 | ||
| Co2 | 22 | MCV | 79.9 | NRBC Abs | 0.00 | ||
| BUN | 10 | MCH | 25.5 | NRBC % | 0.0 | ||
| Creatinine | 0.89 | MCHC | 31.9 | ||||
| Glucose | 114 | RDW | 17.1 | ||||
| ALT (SGPT) | 53 | PLT | 419 | ||||
| AST (SGOT) | 74 | MPV | 10.3 | ||||
| Alkaline Phosphate | 138 | Monocyte % | 10.1 | ||||
| Total Bilirubin | 0.4 | Monocyte Abs | 0.75 | ||||
| Calcium | 9.8 | Neutrophils Abs | 2.68 | ||||
| Total Protein | 8.4 | Neutrophil % | 36.0 | ||||
| Albumin | 4.2 | Lymphocyte Abs | 3.63 | ||||
| Magnesium | 2.1 | Lymphocyte % | 48.8 | ||||
| Phosphorus | 2.6 | Eosinophil % | 4.3 | ||||
| eGFR | >60.0 | Eosinophil Abs | 0.32 |
Additional Lab Findings:
- Troponin T HS < 6 (normal)
- Lipase 3,831 (normal range 0-160 U/L)
EKG:
Normal Sinus Rhythm
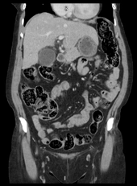
Imaging:
Ultrasound of Gallbladder

CT Abdomen and Pelvis w/o Contrast

Assessment:
D.A. is a 65 y/o F hospital day 4, admitted for sudden, severe 10/10 RLQ pain radiating to the lower back. Patient had tenderness in the RUQ on light and deep palpation with positive Murphy’s sign. Patient is on continuous lactated ringers infusion 125 mL/hr, NPO, receiving Cefoxitin 2,000 mg in dextrose 5% water 100 mL IVPB every 8 hours at 200 mL/hr over 30 minutes. On examination patient is no longer TTP in the RUQ. She has not had a bowel movement or flatus since day of admission. Reports that she is urinating 5-6 times a day and able to ambulate to the bathroom without difficulty. Denies fever, chills, shortness of breath, chest pain, dysuria, urinary urgency, urinary frequency, dysuria, hematuria, vaginal bleeding/discharge.
Plan:
#cholecystitis
- Continue abx: Cefoxitin 2,000 mg in dextrose 5% water 100 mL IVPB every 8 hours at 200 mL/hr over 30 minutes
- IV fluids PRN
- morning labs; note if lipase is trending downwards
- Pending robot-assisted laparoscopic cholecystectomy
#diet/nutritional supplements
- Advance to low fat diet today as tolerated
#pain control
- Ketorolac 15 mg injection every 6 hours as needed for pain; do not exceed 120 mg in 24 hours
#instructions
- Incentive spirometer 10 times per hour while awake
#chronic medical conditions HTN, T2DM, Sjogren’s syndrome, arthritis, osteoporosis, cataracts, and malignant neoplasm of upper outer quadrant of LT breast
- Vital signs monitoring
- Cardiology consult for optimization prior to cholecystectomy